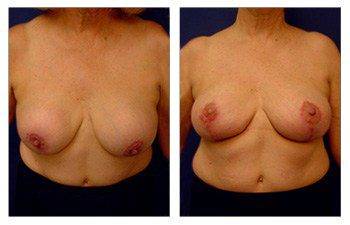
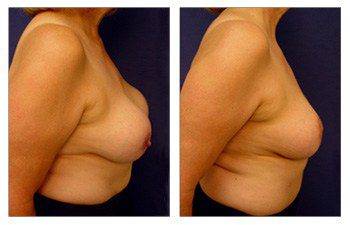
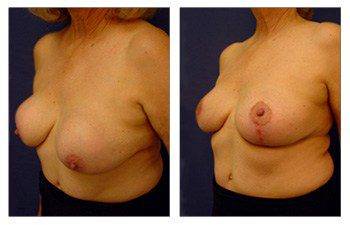

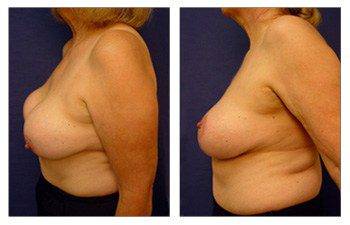
After having breast implants, some women experience capsular contracture. Capsular contracture is when your breast implant gets scarred up and firmed. Visually, a capsular contracture looks like a stuck-in-place breast implant and the breast mound sagging over it. It is possible to improve this with a Breast lift with implant augmentation to correct capsular contracture.
This is also what we call a snoopy deformity. When using silicone implants, the implant gets sticky and may result in this snoopy deformity. In comparison, saline implants will move down with the breast mound and nipple areolar.
A breast lift corrects capsular contracture, and some patients take this opportunity to increase their implant size. When performing a breast lift with breast augmentation to correct capsular contracture, there are two concepts to remember.
a) The first concept pertains to situations where the capsules are not excessively thickened. When dealing with slightly thickened capsules, a surgeon can use them to their advantage when performing a breast lift with implant augmentation.
This can be an advantage to surgeons because, in a breast lift with breast implant surgery to correct capsular contracture, you have to reposition the implants and make room for a larger implant. Suppose the capsules do not exhibit significant thickening. In that case, we can better preserve blood flow, make necessary adjustments to the pocket position, and still utilize the lateral or superior capsule to counteract lateralization.
One example is if the breast lateralizes, you will see the breasts sagging off the chest as you lose the pectoralis area, creating a falling effect of the breasts to the armpit area. In a breast lift revision or a breast lift with implant augmentation to correct capsular contracture, the goal is to centralize and metalize the breasts, sewing the pocket laterally.
Another example arises when implants sag with the breast and areola, requiring a capsulectomy to establish a new chest wall pocket. If the implants become immobile, concerns arise about breast malposition or upward movement. In such instances, we suggest using a breast band.
If you have silicone implants with high breast pockets, the surgeon can strategically employ this method. It retains the superior capsule’s position, preventing the implant from moving upward and eliminating the need for a breast band.
In another scenario, when choosing a larger size, the surgeon must release the previous capsule to create space, requiring a capsulorrhaphy and sometimes a capsulectomy.
b) The second concept is relevant when the capsules become highly thickened to a degree that prevents the breasts from expanding. In this case, your surgeon will have to remove the whole capsule. If this is the case, why not remove the capsule constantly?
The answer is that a somewhat hardened capsule often assists when the skin thins out, potentially exposing the implant. A capsule maintains blood flow to the nipple and possesses vascularity. If it’s possible to preserve the capsule, your surgeon will endeavor to manipulate it rather than remove it, as this is beneficial for maintaining blood flow to the nipple.
A vertical mastopexy is generally employed during a breast lift with implant augmentation. The primary concern is preserving blood flow. This is crucial because back cuts in the procedure can already compromise horizontal blood flow. Additionally, compressing the nipple-areolar area can jeopardize perpendicular or vertical blood flow. Therefore, it is preferable to avoid this risk by retaining the capsule. This careful approach helps ensure the overall success and safety of the surgery.
Here, we present our 58-year-old patient who demonstrates a breast lift with implant augmentation to correct capsular contracture. The patient previously experienced a condition known as «snoopy deformity,» where the implant was positioned high and the breast mound sagged below.